
Longevity, skin‑cancer diagnostics and the need for a bio‑systemic integrative Healthcare vision
Longevity medicine, focussed on extending healthy lifespan and preventing illness is rapidly transforming the foundations of healthcare. This is already visible in fields like dermatology, as skin is a powerful biomarker for systemic aging and skin cancer diagnostics is taking a leap towards continuous monitoring and early detection. However a new bio-systemic integrative vision of healthcare posits that the human body and individual cannot be reduced to the sum of organs, parts and functions and cautions about the risk of overdiagnosis and the ethics of screening.
LONGEVITYMEDTECHHEALTHCARE STRATEGYLONGEVITY BIOMARKERSCANCER DIAGNOSTICSSKIN CANCER
Irene Petre
4/29/20268 min read


Longevity medicine is defined as advanced personalized preventive medicine powered by deep biomarkers of aging and longevity. It integrates biogerontology, geroscience, precision medicine, and AI‑driven diagnostics to detect biological decline before disease manifests. According to a 2024 review, longevity medicine is structured around a “Longevity Pyramid,” where the base layer is early detection and preventive diagnostics, followed by lifestyle interventions and personalized therapies tailored to genetic and phenotypic profiles.
This model reflects a profound shift: instead of waiting for the onset of disease, clinicians increasingly aim to identify risk trajectories years earlier with profound implications for how we deliver healthcare in general and for oncology diagnostics in particular. Skin cancer is one of the best examples.
Dermatology has established itself as a leader in longevity research and medicine
For some time now, most research and clinical practice in longevity have focussed on two key therapeutic areas: neuroscience and cognitive decline (as the areas with perhaps the most investment) and dermatology, which is currently re-branding from "anti-aging" to "skin longevity" - as arguably the most commercially active and public-facing sector of longevity.
The skin is the body's largest organ and a visible mirror of biological age - in fact longevity researchers are using skin-specific epigenetic clocks (like the Horvath clock) to measure how fast a person is aging internally. The skin reflects systemic aging, the skin being a powerful biomarker for the immune function, oxidative stress, metabolic health, environmental factors and cumulative DNA damage.
Skin is very important for aging as chronic low-grade inflammation in the skin (often called "inflammaging") can release pro-inflammatory signals into the bloodstream, accelerating the aging of other organs. Also because it is easier to test topical treatments than internal drugs, many breakthrough technologies (like senolytics and gene reprogramming) are first trialed in skin models.
Key longevity therapies and technologies are revolutionising skin health - from cellular reprogramming (rejuvenating by many years skin cells by using Yamanaka factors) to exposome and stem cell therapies and up to tissue bioengineering - laboratories like those of Mayo Clinic are using 3D bioprinting and "skin-on-a-chip" to study how genetics and the environment are shaping the "skinspan".
Skin cancer is on the rise but skin can be monitored continuously
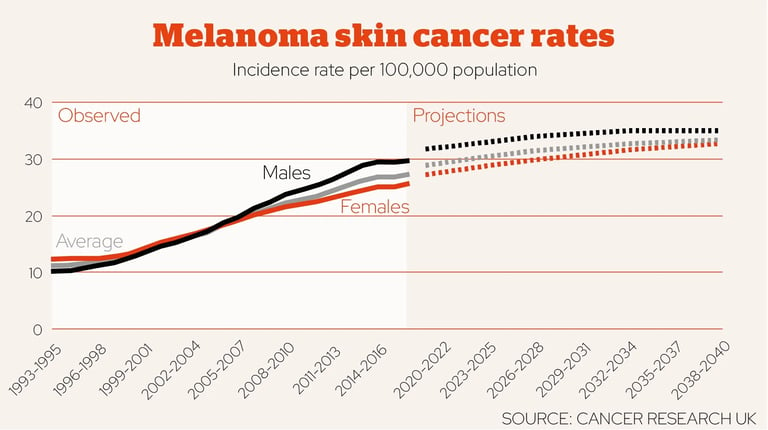
Skin cancer represents the most common malignancy worldwide and its incidence seems on the rise - worldwide and in Europe. The number of estimated skin cancer cases globally is between 1,2 million and over 7 million, with the latter figure being a more realistic estimate according to many scientists. Out of these only c. 500,000 yearly are estimated to be melanoma, but this is by far the most aggressive and deadly form of skin cancer.
Skin cancer is a disease frequently linked to UV radiation exposure, sun burns and tanning beds but also aging and environmental factors. Melanoma in particular is strongly age‑associated: cumulative UV exposure, immune decline, social factors and genomic instability—all hallmarks of aging—contribute to risk.
According to Skin Cancer Foundation and GLOBOCAN, high-risk patient groups include individuals with fair skin, those with many or atypical moles, immunodeficient patients, organ transplant patients and older adults who are more and more often told they would benefit from regular skin check-ups.
The skin is the only organ fully accessible to non-invasive imaging and unlike internal organs it is easier to monitor continuously, using an increasing variety of technologies, from the traditional dermoscopy to reflectance confocal microscopy (RCM), line‑field confocal optical coherence tomography (LC - OCT) and many AI-assisted image analysis tools - including via patient's smartphone captured photos (see DERM tool from Skin Analytics woking with the NHS in the UK). In theory some of these tools allow clinicians to detect microscopic changes long before symptoms appear but in practice things are more complicated - false positives and false negatives appear still often enough due to not high enough specificity and sensitivity rates. New types of tools and a shift in healthcare paradigm would be needed to not just improve on the detection metrics but to start seeing the human body in its systemic entirety, closely linked to the concepts of personhood and its environment.
So skin cancer incidence has risen substantially in many high‑income regions over recent decades, driven indeed by increased UV exposure, pollution, aging but also, paradoxically, by better detection, greater medical surveillance and changing pathology thresholds of the population, which led to overdiagnoses.


Overdiagnosis and the ethics of screening and personal responsibility
As shown skin cancer incidence has been rising for the past three - four decades and whilst there are many biological, environmental and cultural factors at play, greater medical surveillance seems to have been a decisive factor.
Specifically for melanoma, some authors from Denmark and Norway report in 2024 that the degree of overdiagnosis ranges from 29% to 60%. Skin biopsies are invasive and depending on the location of the presumed tumour and dimensions can be painful and inaesthetic for several days or weeks. In case of invasive treatment, surgical excisions and radiation therapy can also leave profound scaring, pain, can cause complications for other parts of the body or adjacent tissues, can cause prolonged fatigues (months or years). This is altering significantly the quality of life of patients whilst some of them do not even have the certainty of their cancer diagnostic.
A hyper focus on early detection can lead to unnecessary biopsies, which can lead to overtreatment and very high costs (both for patients and healthcare systems - a skin biopsy for example costs on average between EUR 500 - 2200 in Europe) coupled with anxiety, pain, scarring, secondary side effects and complications and overall a loss of quality of life, in cases where it wasn't even necessary.
Balancing accuracy, sensitivity and specificity of skin cancer diagnostic tools becomes ethically essential. Longevity medicine must avoid a future where more testing becomes equivalent to better care. There is a fine balance between a healthy effort to prevent and test/screen for disease and "hyper testing" and surveillance like it happened during the Covid-19 pandemic, which led to increased population anxiety, an increase in mental health issues, an overload of the medical system and economic pressures.
Longevity research and medicine also reframes health as a lifelong responsibility by shifting care toward early detection, continuous risk management, and preventive interventions that require sustained individual effort and almost permanent system‑level engagement, which can be burdensome for both patients and clinicians, on constant pressure to keep-up with new discoveries and upskill.
This raises important ethical questions especially in oncology where on one hand early detection can mean the difference between life and death and on the other hand, inaccurate diagnosis and false positives can also have devastating effects, as well as the constant pressure to monitor one’s health in minute detail:
How much responsibility should individuals bear for preventive behaviours?
What obligations do healthcare systems have to provide equitable access to early diagnosis?
How much responsbility can we shift to medical professionals and for which aspects? Should there be a limit to medical knowledge and upskill to prevent errors and burnout?
How should society support those with fewer resources?
Towards a bio-systemic integrative healthcare vision
The challenges of over-diagnosis in skin cancer (and other areas) together with the limitations of personal patient responsibility in prevention and the drawbacks of hyper-screening are calling for a paradigm shift in the curent prevention and early diagnosis models of healthcare, especially in areas like dermatology as skin is much easier to monitor (and panic about) compared to other organs. One such paradigm shift could be the transition to a bio-systemic integrative vision of medicine.
The current bio-systemic integrative vision in healthcare is a paradigm shift away from traditional symptom based-care towards a holistic 4P approach (predictive, preventive, personalised and participatory). This vision positions the human body as a complex biological system in constant interaction with the environment (the exposome). The implication is that treating one organ or one disease in isolation may not lead to the best healthcare and wellbeing outcomes for the individual patient as well as the realisation that not all diagnostic tools and diagnoses can be suitable for all patients - context (such as different environmental factors, genetics, lifestyle, culture, mindset) matters a lot.
According to Prof. A. Carrara from Ateneo Pontificio Regina Apostolorum, there are currently four contemporary paradigms of longevity medicine, ranging from the mechanistic "body as a complex machine" one (where aging is just wear and tear that needs repair) and up to the bio-systemic integrative paradigm that posits that the living body cannot be reduced to parts, functions or emergent properties and must be seen as a unitary system where biological, psychological, social, environmental and spiritual dimensions are merging.
H.G. Eilenberg and J. Slatman argue that embodied lived experiences and embodied identity may change with aging, but it is not a given for all individuals and not all aging people change in the same way. Each living person, body, organ and cell is in a continuous system transformation and exchange with the environment – this cannot be easily predicted just through AI mathematical models and people do not all age the same. Their different embodied lifelong experiences call for qualitative, phenomenologically informed methods in ageing research and for policies that respect older people’s diverse embodied perspectives.
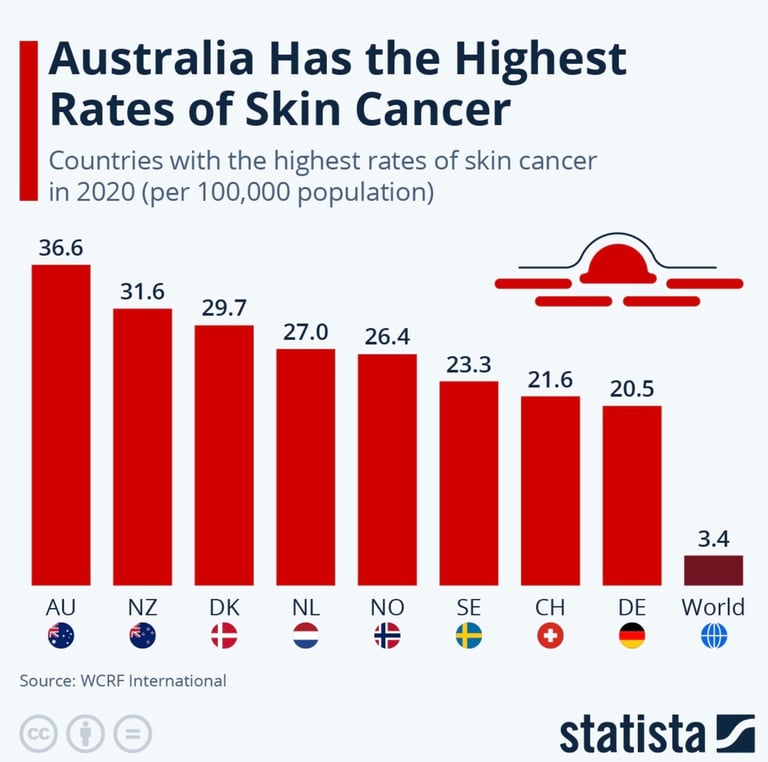
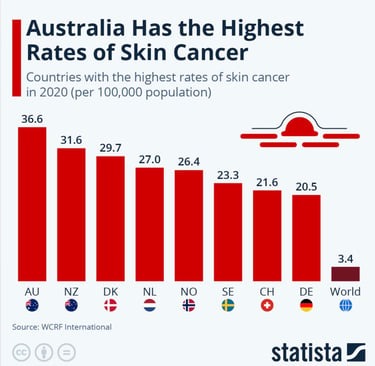
Finally, not all aging patients have the same economic means to prevent, not all bodies allow for the same aging process, some people's environments would predispose to one illness or another, beyond individual responsibility - for example Australia and New Zealand have the highest incidence of skin cancer due to high ambient ultraviolet (UV) radiation levels, an outdoor lifestyle and a large population with fair skin prone to sun damage:
In conclusion...
Multiple peer‑reviewed analyses conclude that the rise in skin‑cancer diagnoses since the 1970s is partly driven by greater medical surveillance (more screenings, more biopsies, and more diagnostic scrutiny), which has increased detection of indolent lesions and likely produced some overdiagnosis — this effect is strongest in high‑income/developed countries where access to dermatology and cancer screening is greater.
Dermatology and skin care have been at the forefront of longevity research for several years and the ever growing concer with skin appearance, hyper health surveillance and strong focus on prevention are likely to conduct to overdiagnoses of skin cancer, over-medicalisation and increased patient and social anxiety – an obsession with disease prevention and health improvement. A new bio-systemic integrative healthcare paradigm is likely to help balance these processes, highlighting that the human body cannot be infered through AI mathematical functions alone and that to effectively improve quality of life for skin cancer patients – the mathematical data perspective needs to be coupled with in-vivo biological processes, genetics, external environmental conditions, social and psychological aspects, lifestyle and culture.
Some sources:
American Cancer Society, ‘Basal and squamous cell skin cancer: causes, risk factors and prevention’, American Cancer Society, 2024
Arnold M, Singh D, Laversanne M, Vignat J, Vaccarella S, Meheus F, et al., Global burden of cutaneous melanoma in 2020 and projections to 2040, JAMA Dermatology, 2022
Celi LA, Fine B, Stone DJ, An awakening in medicine: the partnership of humanity and intelligent machines, Lancet Digital Health, 2019
Cirillo N, Global epidemiological trends in the incidence and mortality for melanoma, Skin Health and Disease, 2025
Eilenberg HG, Slatman J, Four modes of embodiment in later life, Journal of Aging Studies, 2024
Fiandaca M et al, Systems healthcare: a holistic paradigm for tomorrow, BMC Systems Biology, 2017
International Agency for Research on Cancer (IARC) / GLOBOCAN, Melanoma of skin — fact sheet, GLOBOCAN 2020
Martinovic A et al., Climbing the longevity pyramid: overview of evidence-driven healthcare prevention strategies for human longevity, Frontiers in Aging, 2024
National Center for Biotechnology Information (NCBI Bookshelf), Radiation and the skin (Radiation Injury chapter), Overall Evaluations of Carcinogenicity: An Updating of IARC Monographs Volumes 1 to 42, NCBI Bookshelf, 1987
Scott AJ, The longevity society, The Lancet Healthy Longevity, 2021
Skin Cancer Foundation US, Basal Cell Carcinoma Risk Factors , accessed 27 April 2026 (updated April 2026)
Zhavoronkov A, Mamoshina P, Vanhaelen Q, Scheibye‑Knudsen M, Moskalev A, Aliper A, Artificial intelligence for aging and longevity research: recent advances and perspectives, Ageing Research Reviews, 2019
Zhou L, Zhong Y, Han L, Xie Y, Wan M, Global, regional, and national trends in the burden of melanoma and non‑melanoma skin cancer: insights from the Global Burden of Disease Study 1990–2021, Scientific Reports, 2025
...and many others
Feel free to reach out to us if you are interested in the subject or would like to know more about our services.
IGEA Healthcare
Strategic Advisory for Life Sciences
Switzerland, UK, Italy
contact@igeahealthcare.com
© 2025 - 2026. All rights reserved.