
AI alone is not enough in Skin cancer diagnostics – we need in-vivo data and hybrid tools for better accuracy and patient trust
The quest for early detection and prevention drives the rise in AI -assisted skin cancer diagnostics, but nature’s complexity still beats AI only ex-vivo models. Skin cancer diagnoses have been on the rise for the past five years, not only due to environmental and lifestyle changes but also due to an increase in screening and over-detection. Traditional diagnostic methods as well as AI only tools tend to have low accuracy, often due to low specificity, producing higher false positive results. Hybrid tools, combining AI with in-vivo tissue, cell and molecular information at the same time can generate better outcomes in skin cancer and in other oncology areas, moving us closer to a systemic medicine approach.
MEDTECHSKIN CANCERCANCER DIAGNOSTICSHEALTHCARE INNOVATIONSYSTEMIC MEDICINE
Irene Petre
6/11/202612 min read


Skin cancers on the rise – UV exposure, pollutants and increased testing and medical surveillance lead to growing incidence
Skin cancer incidence seems on the rise - worldwide and in Europe. It is a disease frequently linked to UV radiation exposure, sun burns and tanning beds but chemicals from air and water pollution (1,2), cosmetics and food (3), can also contribute to skin cancer, especially inorganic arsenic and PAH/coal-tar exposures (4) n smaller proportions compared to UV exposure.
According to Skin Cancer Foundation and GLOBOCAN, high-risk patient groups include individuals with fair skin, those with many or atypical moles, immunodeficient patients, organ transplant patients and older adults who would benefit from regular check-ups (5, 6, 7). More exposed geographic areas include the Nordic and Western countries in Europe, the US, Australia and New Zealand (8,9). In fact Australia has the highest incidence rate in the world standardised by age (ASR per 100,000 population) with an ASR of 37 for melanoma and nearly 17,000 new cases in 2022, due to poor quality of its ozone layer. It is followed by Denmark with 3144 cases/year and an ASR of 31,1, then Norway with similar numbers and New Zealand with an ASR of 29,8 and over 2,700 new cases yearly (9). Other countries in Europe such as Finland, Netherlands, Germany rank high as well.
Whilst the mortality is highest in melanoma (case fatality is about 20% compared to non-melanoma case fatality of c. 5% (10) versus other non-melanoma skin cancers (NMSC), the melanoma cases are low (c. 350,000-500,000 global cases yearly) compared to NMSC (estimated between 1,2 million and 7 million (11) cases globally and c. 27% in Europe). The incidence of melanoma and overall skin cancer is set to see strong growth in the coming 10 – 20 years and more penetration among younger people due to behavioural and environmental changes: increased use of indoor tanning beds, travel and sun exposure and increased ozone/UV variability in some geographic areas (12, 13, 14).
Skin cancer incidence has risen substantially in many high‑income regions over recent decades, driven indeed by increased UV exposure, pollution, aging (15) but also, paradoxically, by better detection, greater medical surveillance and changing pathology thresholds of the population, which led to over-diagnoses (16, 17).
A vast majority of skin cancer biopsies in the US, Europe and other developed countries are negative: A study of over 80,000 biopsies published in the JAMA Dermatology in 2017 found that 83% of them were benign (18) and a more recent study in 2025 (19) found that only 13,4% out of nearly 13,000 biopsies analysed, were actually histologically melanoma. This reflects a greater anxiety of our society and our healthcare systems in developed countries over improving skin cancer diagnosis (or any cancer diagnosis) and building detailed patient records, but also highlight low accuracy rates of many mainstream diagnostic tools used.
Specifically for melanoma, some authors from Denmark and Norway report in 2024 that the degree of overdiagnosis ranges from 29% to 60% (20). Skin biopsies are invasive and depending on the location of the presumed tumour and dimensions can be painful and inaesthetic for several days or weeks. In case of invasive treatment, surgical excisions and radiation therapy can also leave profound scaring, pain, can cause complications for other parts of the body or adjacent tissues, can cause prolonged fatigues (months or years) (21, 22, 23, 24). This is altering significantly the quality of life of some patients and some do not even have the certainty of their cancer diagnostic.


Cost pressures and the need for accurate early detection drive the quest for new diagnostic tools
Given the current financial strain on Healthcare budgets in Europe and elsewhere, cost remains a key consideration for clinics, hospitals and the healthcare system. Some traditional testing methods such as the biopsy (still the gold standard in skin cancer testing) can be very expensive for the patient and not the most effective tool for hospitals - currently 83% of biopsies come back negative (18). Newer technologies such as RCM and LC-OCT are also expensive to acquire by smaller clinics and hospitals in Europe and procurement is complicated and costly.
The cost of a typical skin biopsy in Europe varies by country, type and complexity, from c. EUR 400 on the low end to over EUR 2000 on the high end (26). Other widely adopted triage methods include dermoscopy, histopathology and immunohistochemistry and some image diagnostics methods such as reflectance confocal microscopy (RCM), Line-field Confocal Optical Coherence Tomography (LC-OCT) or molecular diagnostics (e.g. gene expression analysis). The Viva Scope 3000 (a hand-held RCM device) can cost c. EUR 150-200k and the better version 1500 with larger imaging field costs around EUR 180k – 300k, and the deepLive LC-OCT (27, 28, 29) and similar systems are equally expensive, making these newer technologies often unaffordable by smaller clinics in Europe. A compound problem is that clinics and hospitals usually need to pay then extra money for installation, training, warranty, software, VAT, local distributor margins where applicable etc. which can represent another 20% - 60% on top.
For early prevention clinics anywhere in the world need to be able to also perform effective early detection – so apart from cost, it rests the problem of variable accuracy rates of more mainstream tools – for example dermoscopy, a more cost-effective tool, only has a specificity rate of c. 49% (so it produces more false positives) (30), despite high sensitivity (circa 97%). Therefore dermoscopy remains a simpler and limited diagnostic tool, much dependent on the skill of the physician using it (31). Governments’ reimbursement interest in early prevention in countries like the US, UK or some European countries drove the rise in AI led skin cancer diagnostic tools.
The US FDA cleared multiple AI-assisted software platforms (32, 33, 34) from MelaFind (of Mela Sciences, a start-up) at the end of 2011 to the AI assisted dermoscopy software 3Derm Systems and DERM of Skin Analytics in 2024 - Skin Analytics is in fact a British startup in melanoma diagnostics using smartphone taken images and widely partnering with the NHS England since 2020 (it claims to have successfully screened over 170,000 patients and caught over 15,000 cancers (35, 36). Additionally, in the EU Philips Healthcare's IntelliSite Pathology Solution received CE mark for melanoma whole-slide image analysis in 2024, enabling remote pathologist review of digitised skin biopsy specimens and reducing turnaround times for Breslow thickness assessment, the test that predicts survival rates for localised melanoma (37).
The issue of variable accuracy rate persits across some new AI tools as they seem to have lower accuracy than initially expected in countries and populations with higher skin cancer prevalence. Lower accuracy is linked to lower sensitivity (this is the true positives rate) of some methods and lower specificity (this means a test’s ability to identify true negatives compared to all actual negatives). For example Mela Sciences withdrew its main AI led product, MelaFind in 2017, after five years of commercialisation in the US and other countries due to lower accuracy in the real world compared to the clinical trials. Despite very high sensitivity in its pivotal trials, its low specificity produced many false positives in practice - regulators flagged software/labelling issues and commercial uptake was poor due to cost and workflow limits (38, 39). However, accuracy alone can be a misleading KPI when disease prevalence is low. Oncologic diagnostic tools should also be able to apply different decision metrics depending on the type of cancer: for example, sensitivity should be prioritised when screening for a deadly but treatable disease, whilst specificity should be prioritised when doctors want to avoid false alarms that can cause harms, patient anxiety, unnecessary treatments and high costs. Higher accuracy is not always important but in higher disease prevalence areas it is important and it can be linked to both test sensitivity and specificity.
So far innovation in skin oncology has been heavily driven by the need for speed, early detection and cost reduction. Non-invasiveness and reducing procedure discomfort for patient are other important considerations and as new technologies develop they take these design principles increasingly into account.
Apart from potential lower accuracy, AI only led diagnostic tools present other shortcomings
New purely AI led solutions suffer from a few notable shortcomings including (but not limited to):
- often poor transparency and explainability (the so called “black box outputs”), where doctors do not fully understand how AI made a decision or put a diagnostic
- algorithmic bias and inequity – most models are likely to be trained on datasets from light-skin patients, so they are less sensitive on darker skin patients, which can lead to missed cancer diagnostics and increased health inequity; on white skin patients the AI-led tools can lead to overdiagnosis, patient anxiety and unnecessary costs
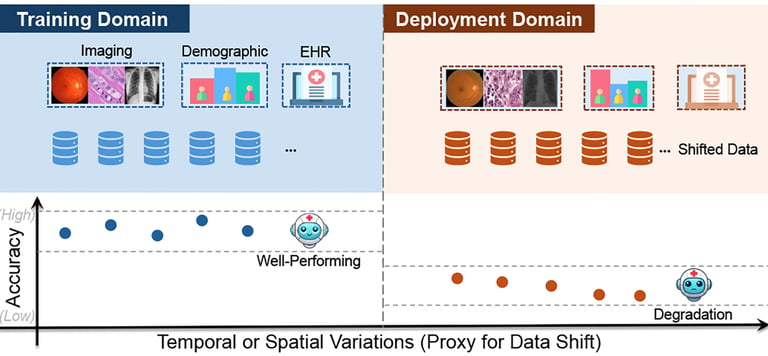
- dataset and model drift over time (40, 41) – data drift/shift refers to a change in the statistical distribution of features or inputs in real world compared with the training data and can happen when the model is deployed on different devices or skin types compared to the training data, which can lower accuracy; model drift refers to a change in the conditional relationship (such as changes in practice or the hardware) so the AI model’s learned mapping is no longer valid;
- model degradation and lower accuracy (41, 42) – is the observed outcome (falling metrics – e.g. lower accuracy rates) and when it happens it is difficult to assess if the cause is dataset shift, model drift, labelling issues, code errors and bugs etc.
- undermine clinical authority and accountability at the same time as both patients and clinicians may defer to AI outputs (algorithmic authority) even when inappropriate (due to lack of time, lack of expertise or lack of visibility over how AI outputs were generated), shifting responsibility from doctors and clinics to medtech manufacturers, distributors, IT developers or simply to the AI system itself and thus eroding clinical judgement over time and patient trust in clinicians
- intellectual property and model provenance (43) — third‑party training data or licensed models can create complex IP disputes
- integration and interoperability failures (44) - poor EHR/API integration can break workflows, cause data loss and create unsafe situations for patients; in fact current diagnostic pathways in most national healthcare systems rely on fragmented and poorly integrated data.
Hybrid tools that combine AI algorithms with in-vivo tissue, cell and molecular data can offer better accuracy and patient trust
In order to avoid some of these challenges with accuracy, eliminate opaque black-box outputs, empower physicians and improve clinical knowledge and patient trust – new diagnostic tools are required. Tools that combine AI with real world in vivo tissue analysis, presenting skin specialists with varied analyses and inferences, thus empowering them to make more informed decisions about diagnostics and treatment selection, rather than letting a sole AI tool put a diagnostic. Combining in-vivo tissue analysis with multimodal AI-assisted data integration in oncology is likely to produce better outcomes in the future believe some experts (45). AI systems synthesize multimodal inputs combining imaging, molecular markers and clinical patient data—to improve diagnostic precision and support early disease detection (46). Biological responses from tissue studies, combined with clinical patient data from medical records and possibly with genomic profiles will provide dermatologists and oncologists with valuable insights and empower them to make the right decisions in skin cancer diagnostics but also in regenerative therapies (46).
Some new medical technologies are making inroads to integrate various dimensions of the biology of molecules, cells and tissues together – spatial omics for example looks set to revolutionize pathology by measuring physical tissue structure and molecular characteristics at the same time, in real world (47) but it is debatable if new AI models using ex-vivo data can fully capture and correlate correctly the complexity and physiology of human organs at their cellular and molecular level. These change their state all the time, in real time, in ways not fully understood by scientists and algorithms yet.
Therefore ex-vivo tools could be complemented by integrating in-vivo information (48) in what is called hybrid diagnostics, which helps getting a better understanding of the human body and help establish trust between the clinician and patient since the patient can be reassured that multiple personal data points are being used and that the clinician makes their diagnostic using the patient's real time biological information and not relying solely on ex-vivo exploratory data and AI only diagnostics. However these hybrid tools and AI technology itself are still in their infancy in the medical field and more research is needed.
New hybrid tools using in-vivo patient information are not without ethical challenges
Trying to understand human body physiology and define what health means through simply ex-vivo AI -led data and tools may be fallacious. The human body is a lot more than the sum of its organs and parts, its mechanisms are not fully understood and our health (including the onset and evolution of cancer) is intrinsically linked to our environment, mind, emotional states, in a new (or re-emerging) systemic integrative vision of medicine (coined as systemic medicine). This vision spans prevention, diagnostic and treatment and the degree of patient freedom of choice across these three dimensions. The technocratic view of “human as a machine” or “body as a machine” is a mechanistic metaphor in medicine that separates organs and parts from the whole body physiology (49, 50) and which is not the best model for understanding human health.
Thus a more complex biological, psychological, social and cultural multi-disciplinary approach is needed (not just for diagnosis but also for treatment) - an approach focussed on accounting for the multiple dimensions of disease and which incorporates real-time in-vivo changes. AI can help but it is not advisable to make it the primary decision maker in skin cancer diagnostics (or in other medical decisions).
Incorporating in-vivo information into new diagnostic tools can bring real-world real-time data - including "as it is" characterisation data - into the equation and help clinicians make better decisions. This way clinicians are not relying solely on algorithmic correlations an AI-only tool makes based on past data from datasets it was once trained on - datasets which may anyhow become outdated or suffer from other flaws.
But ethical challenges remain around data privacy - especially re-identification risks , around commercial exploitation and clinician over-reliance on AI outputs when incorporating in-vivo patient biological data.
Even when data is ostensibly anonymised, integrating multi-omic and in-vivo imaging data can make patients vulnerable to re-identification and using patient genomic and cellular data for AI creates the risk of corporate patient data commodification, using patient data without explicit ongoing consent for future purposes. Also if If clinics rely solely on AI to synthesize in-vivo and molecular data, human dermatologists and pathologists may lose their capability to independently recognize complex cellular nuances and rare presentations (51).
Therefore multimodal uses of patient data, standardised and regularly updated informed consent protocols, improved clinician training and ethical AI design choices are likely to help if implemented in a responsible way.
Some sources:
https://monographs.iarc.who.int/agents-classified-by-the-iarc/
https://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-causes-and-risk-factors/
https://gco.iarc.who.int/media/globocan/factsheets/cancers/16-melanoma-of-skin-fact-sheet.pdf
https://gco.iarc.who.int/media/globocan/factsheets/cancers/16-melanoma-of-skin-fact-sheet.pdf
https://www.wcrf.org/preventing-cancer/cancer-statistics/skin-cancer-statistics/
https://gco.iarc.who.int/media/globocan/factsheets/cancers/16-melanoma-of-skin-fact-sheet.pdf
https://www.jaad.org/article/S0190-9622(23)00518-2/abstract, https://pmc.ncbi.nlm.nih.gov/articles/PMC11703817/
https://jamanetwork.com/journals/jamadermatology/fullarticle/2790344
https://newsroom.uw.edu/news-releases/most-mole-biopsies-are-benign-says-text-analysis-emrs/
https://costdigest.org/biopsy-cost-insurance-price-range-budget/
https://www.medicalexpo.com/prod/caliber-imaging-diagnostics/product-104256-725741.html
https://www.vivascope.com/us/instant-optical-biopsy-in-vivo/vivascope-1500-3000-combo/
https://pmc.ncbi.nlm.nih.gov/articles/PMC11818986/#:~:text=Pooled%20sensitivity%20and%20specificity%20of,could%20improve%20their%20detection%20rate
https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfRES/res.cfm?id=136172&
https://pmc.ncbi.nlm.nih.gov/articles/PMC11180084/?utm_source=copilot.com
https://pmc.ncbi.nlm.nih.gov/articles/PMC10655164/#:~:text=Open%20in%20a%20new%20tab,%2Dscale%20patient%20screening%20(E%2DF. - dovrebb essere source 41?
https://www.dermatologytimes.com/view/derm-dispatch-navigating-the-ethics-of-ai-assisted-dermatology
Feel free to reach out if you would like to know more about the subject or about our services.
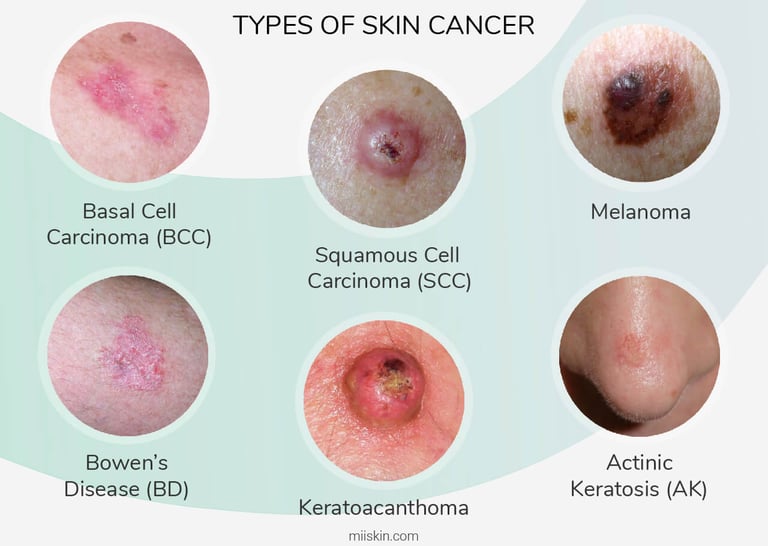
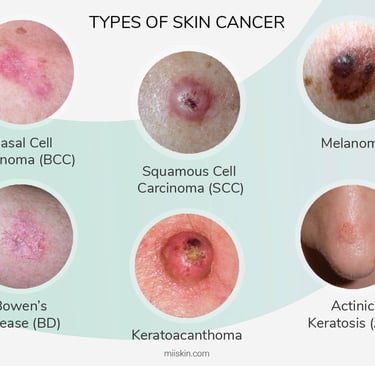
Most common types of skin cancer
Illustration of performance degradation of medical AI models under temporal or spatial variations (see source 42)
According to research, tanning beds contribute to skin cancer
IGEA Healthcare
Strategic Advisory for Life Sciences
Switzerland, UK, Italy
contact@igeahealthcare.com
© 2025 - 2026. All rights reserved.